


Treatment for Children’s Constipation without Miralax
In January of this year the FDA announced it would fund research into the safety of the very popular constipation medication Miralax.
Though Miralax has been approved for use in adults and adolescents for less than 7 days, it has never been approved by the FDA for use in children. Despite this Miralax has been a mainstay treatment by conventional pediatricians for use of constipation in children.
Polyethylene glycol 3350 (PEG 3350) is the active ingredient in Miralax. Just so we are on the same page, ethylene glycol – or antifreeze – is not the same as polyethylene glycol. Though polyethylene glycol is simply a string of ethylene oxide molecules, it is supposedly non-toxic and non absorbable, having no effect other than to loosen stool (poop).
So what’s the problem? The problem is that when the FDA tested batches of Miralax they found small amounts of actual antifreeze: ethylene glycol and diethylene glycol. Not to mention that intestinal absorption of Miralax has never been studied in children, which is very concerning. The FDA has even received reports of psychiatric problems linked to the use of Miralax – specifically tics, tremors and obsessive-compulsive behavior. This would suggest that at least some component of PEG 3350 is systemically absorbed, and we are not sure what the long term consequences are.
I’ve seen countless kids in my office with a chief complaint of chronic constipation, many of whom have seen conventional pediatricians and walked away with a prescription for Miralax. I’m not blaming them – Miralax works extremely quickly and is an easy recommendation to make (we know it will work!) – but it also fails to truly address the underlying cause of why a child is constipated.
One of the main principles of naturopathic medicine is called “Tolle Causem” or Treat the Cause. For kids to have permanent change in their bowel habits we first need to find out why they were constipated in the first place. Read on!
First – how do we know they are constipated? What “counts” as constipation?
Here’s a little guideline of what is normal for kids:
- Babies 1 week old or less usually have 4 or more bowel movements (poops) each day. They are usually liquidy or extremely soft.
- Babies 3 months old or less can have bowel movements as often as several times per day, or as infrequent as once per week. Breastfed babies tend to have less frequent poops because breastmilk is highly absorbable, which doesn’t leave much “left” to make a poop with. If babies are very uncomfortable when passing stool (poop) then I still consider them to be constipated even though it is technically normal to go up to a week. (If it is bothering them, I think it is a problem!)
- By age 2 most children have at least 1 bowel movement per day. They should be easy to pass, formed, no blood in the stool, not pellet-like. Though it is “normal” for kids to skip a day in between bowel movements, I aim for 1 per day. (1,2)
If your child doesn’t meet the guidelines listed above, or is having painful stools or behavior changes around the time of defecation, then I would consider them to be constipated. Rather than just give a laxative, let’s try to figure out why they are constipated.
Lack of dietary fiber
This is by far the most common cause of constipation I see in my office.
To understand why fiber works we have to understand a little about the anatomy and physiology of the intestines. Food is supposed to be digested by the stomach and then further digested and absorbed in the small intestine. Everything that can be absorbed should be by the end of the small intestine – everything else gets dumped into the large intestine. Dietary fiber forms the bulk of “food” that cannot be digested and absorbed – this leaves extra material for the large intestine (or “colon”) t0 squeeze together and form into stool (poop). This dietary fiber is incredibly important because it is what the good gut bacteria (“happy bugs”) live off of. These “happy bugs” provide lots of awesome nutrients for our colon and help regulate our immune system. They also help stimulate the nerves that squeeze the colon and physically push out a poop.
No fiber = nothing for the colon to push against! No fiber = no happy bugs. (No happy bugs = unhappy immune system and no stimulation of the nerves.) No fiber = no poop!!!
The general recommendation is for children to consume 5-10 grams of fiber per day plus the child’s age. 3) (e.g., a 2 year old should have 7-12 grams of fiber.) That’s great, but most families have absolutely no idea what that means.
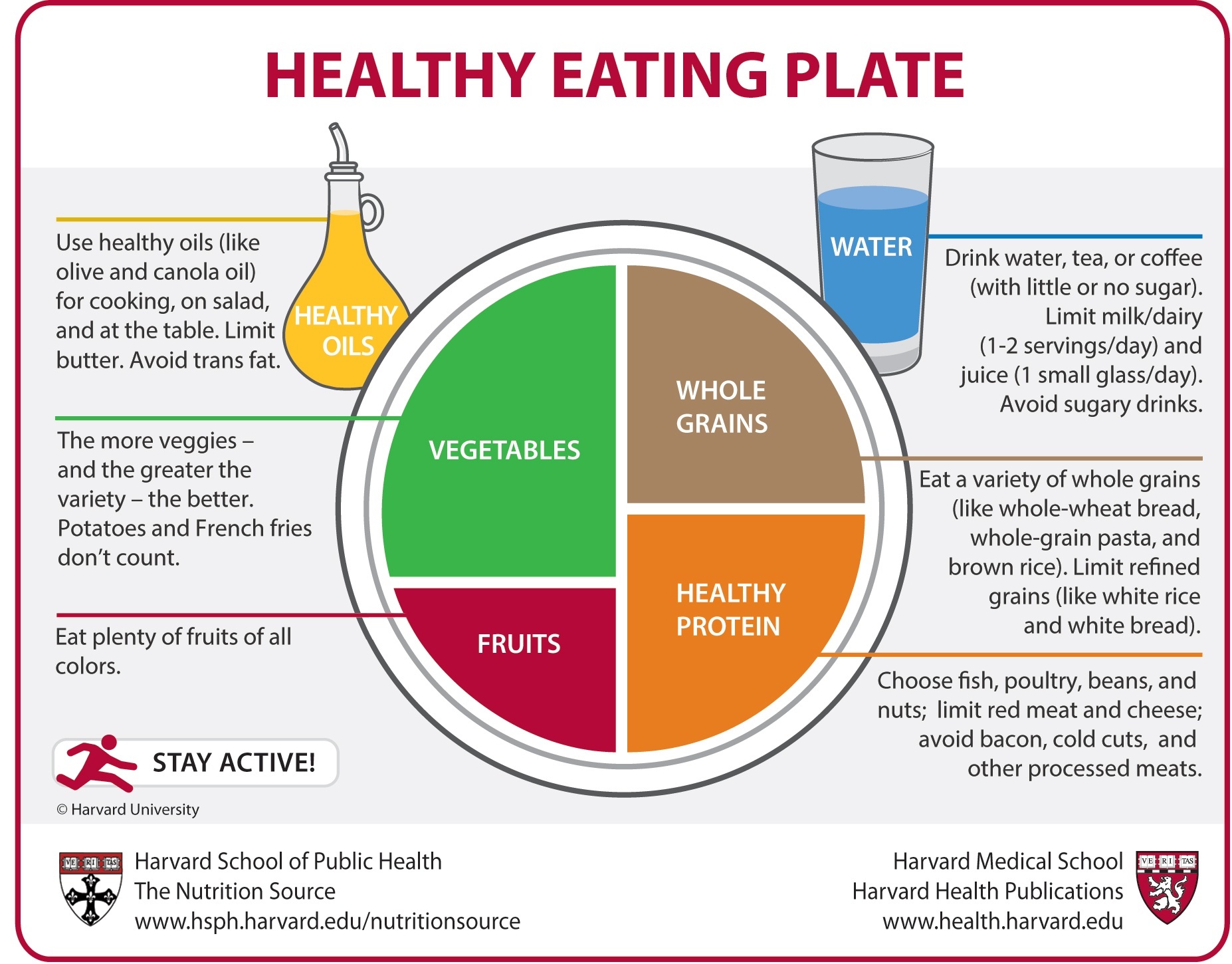
In my office I like to do a drawing of a plate – here we can use the image from Harvard Public Health. The most important thing to notice about the plate is that half the plate is fruits and vegetables. If you are making macaroni and cheese as your main dish (or falafel, or rice and beans, or quinoa and chicken, or chicken nuggets, or hot dogs, or whatever) – your main dish should fill up no more than half the plate. The other half needs to be filled with fruits and vegetables! This is the easiest way to guarantee having enough fiber.
The other method I like to use in my office is to write a side-by-side list of all the foods the child is eating in a day, comparing constipating foods to non-constipating foods. If the constipating foods list is longer than the non-constpating foods list then we have a real problem.
Your child should eat equal number of servings of constipating and non-constipating foods in order to have normal bowel movements. Here is an example chart of all the foods a 3-year old ate in a day:
| Constipating Foods | Non-Constipating Foods |
|---|---|
| Banana | Oatmeal |
| Bread and creamy peanut butter | Carrot sticks |
| Burrito with tortilla and cheese | Lettuce |
| Meat | Frozen berries |
| Pasta | |
| Milk | |
| Cheddar crackers |
See your physician for help going over a list of constipating vs. non-constipating foods, or check out the full list of foods in the Pediatric Constipation Handout in our e-book/e-handout store.
Please note that I do not recommend over-the-counter fiber supplements like metamucil or fiber gummies to increase fiber. Dietary fiber needs to come from the diet – not supplements! Also, I see a lot of kids (and adults) have bad reactions to wheat-based fiber supplements like metamucil. We know that some sensitive kids and adults can end up with Irritable Bowel-like symptoms from use of wheat-based fiber supplements.
Lack of hydration
Drink, Drink, Drink! Yes, yes yes! When you increase fiber it will automatically draw water with it – this means that kids who are increasing their fiber intake need to drink more than they did before. Without increasing water intake there is a chance that increasing fiber will actually make constipation worse!
Make sure your child is not consuming any caffeinated beverages (sodas, energy drinks or coffee drinks). Kids should drink 4-8 cups of water per day – preferably one big glass with each meal.1) Kids who are dehydrated may need to simply drink more water in order to have their constipation improve.
Eliminate Food Intolerances
The first food I recommend eliminating is cow’s dairy. We know that greater than 1 in 3 children with constipation are dairy sensitive. 4) Kids with dairy sensitivity are more likely to have a runny nose, skin rashes and asthma than other kids. 5) If this is your child I highly recommend switching to a non-dairy milk like Almond, Flax, Hemp or Rice milk. (I do not recommend soy milk unless it is in rotation with other dairy-free milks, as there is a concern that the phytoestrogens in soy could alter hormones in both boys and girls.)
Remember that even in non-sensitive kids excessive cow’s milk intake will lead to constipation eventually. Kids need no more than 1 cup of milk three times per day to meet calcium requirements (and there are lots of other ways to get calcium that are dairy-free). That translates to 1 milk for each meal. I often see problems with kids who sip on cups (or sippy cups) of milk throughout the day. Remember that excessive cow’s dairy can also cause iron deficiency anemia, which is a huge problem for development. 6) (Iron deficiency anemia can be hard to detect in kids; sometimes the only symptoms are behavioral problems, ADHD, or problems in school.)
Next frequent food intolerances include gluten, soy, eggs, yeast, bananas, nightshades and corn. For more information on how to do a food elimination challenge/diet please see the Naturopathic Pediatrics Elimination/Challenge Diet Handout.
Stimulate normal peristalsis
Peristalsis is the movement of the entire gastrointestinal system from “top” to “down” (esophagus to rectum). It is what pushes food in a downward direction. Peristalsis causes the intestines to squeeze in a normal snake-like manner, so that a lump of food travels through the tube. See an awesome video of peristalsis in the large intestine.
Children with constipation often have – or develop – abnormal peristalsis. The normal “wave” that should push food down and out in a bowel movement becomes impaired, which makes it difficult to defecate.
Things that stimulate normal peristalsis: probiotics, especially high-dose probiotics. Probiotics have been shown in infants to increase number of evacuations per day and reduce colic. 7) Specifically L. reuteri has been shown to be helpful in infants. For older children and adults probiotics have been shown to speed transit time of the gut (how fast things move through our intestines), and reduce constipation. 8) For older children and adults Bifidobacteria have been shown to be most helpful.
Remember that most over-the counter probiotics are notoriously terrible – many brands have been studied and were shown to contain no active, alive strains – or worse, some were shown to have the wrong strain of probiotic. The only brands I recommend are Pharmax HLC series (HLC neonate, HLC high potency, or HLC intensive. There are also other specific HLC strains), Seroyal/Genetra HMF series, Culturelle, or Klaire Labs probiotics (Ther-Biotic infant, Ther-Biotic child, Lactoprime Plus SCD compliant probiotic, or ABx support). Personally I use Klaire Labs probiotics in my practice, either Ther-Biotic infant, Ther-Biotic child, or Lactoprime Plus if we suspect gut dysbiosis or SIBO. I have no affiliation with the company.
Because probiotics have so many other truly beneficial effects – possibly preventing colds & flu’s, preventing asthma, decreasing allergic responses – I highly recommend this therapy.
Other options:
Ginger has been shown to speed gastrointestinal motility. 9) Older children can take over the counter ginger capsules, younger children can try ginger chews or ginger tincture drops – but please consult your physician for dosage guidelines and safety. Ginger can (and often does) cause upset stomach or burning, and definitely should be used under physician guidance.
Acupuncture has also been shown to improve constipation by speeding gut motility. 10), 11) Acupuncture is helpful for so many things, especially relaxation and decreasing the “nervous” response. Make sure to find an acupuncturist who is very experienced with children.
Herbs which are under the category “Bitters” can also be helpful for atonic constipation. Herbal bitters like Yarrow, Gentian, Blue Flag, Dandelion, and Berberine-containing herbs (like Oregon Grape and Berberis) may all be helpful. Please please consult an experienced herbalist or naturopathic physician – most bitters are contraindicated in pregnancy, breastfeeding and early infancy, and can cause significant harmful side effects if dosed improperly. When used properly these herbs can be very powerful, however. They should be administered in drop doses, preferably mixed in a synergistic formula.
Bowel Retraining
Bowel retraining is the most important step in permanently curing constipation. Bowel retraining involves changing behavior and stimulating normal peristalsis at normal times of the day.
Have your child sit on the toilet at least daily. 1) (Some physicians recommend several times per day, preferably after meals.) At a minimum I recommend setting the child on the toilet at the same time each day, preferably in the morning (either upon waking or after breakfast). It is normal and physiologic to wake up and need to have a bowel movement – I prefer to encourage a morning bowel movement to mimic nature as closely as possible. This is especially important for school-aged children who often hold stools during the day to avoid using a public bathroom.
Here is the key: toilet time must be highly reinforced with positive encouragement and rewards. It must be a positive experience each and every time the child sits on the toilet. Oftentimes children need to be bribed or rewarded heavily – use sticker charts, reading favorite books, favorite treats/snacks, watching TV or playing games on the phone – whatever works. (It’s okay to throw out the “parenting rules” a little bit – at least at first.) Remember that many kids have very negative associations with the toilet when they become severely constipated, and we need to completely change that association. Make sure to not punish the child for bathroom accidents or inability to have a bowel movement.
Stimulating a bowel movement as a part of bowel retraining
Obviously I prefer to not use laxatives in children, but many times it is necessary to artificially produce a bowel movement to get the bowel retraining process going. There are several options here (starting with the least invasive, least force):
1. Physical activity and knee-to-chest positions. This has not been shown in children, but in older adults physical activity has been correlated to a decrease in constipation. 12) Overweight children and adults are more likely to have constipation, possibly due to lack of exercise and poor parasympathetic tone. General exercise is key here (get them up and running around). For younger children you can sometimes stimulate a bowel movement by placing the child in a knee-to-chest position, which places pressure on the bowels and relaxes the rectum/anus.
2. Castor oil abdominal massage. Abdominal massage has been shown to improve constipation in disabled children. 13) It is gentle, feels great, and is a wonderful bonding time. Dr. Harpster wrote an excellent article here about how to do a castor oil tummy massage for your little one. Castor oil has a mild laxative effect when used topically (do not give internally to children, castor oil is considered a “cathartic” and stimulates a massive, sudden, and often painful bowel movement). Any over-the-counter castor oil is fine.
3. Prune juice or other sorbitol-containing juice. Prunes are high in fiber, but it is actually the sorbitol content that makes them a mild laxative. 1) Sorbitol is a sugar alcohol (but not alcoholic – no worry about giving this to your child) and is absorbed very slowly by our intestines. Sorbitol tends to draw water into the gut which relieves constipation. You can do over-the-counter prune juice (organic please), or try Fruit-Eze paste. Remember that kids with gut dysbiosis will tend to worsen on sugar alcohols like xylitol or sorbitol – if that is your child then I highly recommend contacting your naturopathic physician for a stool test.
4. Magnesium citrate or magnesium glycinate as a laxative. 1) If stools are still not soft enough to have a bowel movement then it may be time to consider a laxative to help get the process started. I typically recommend magnesium powder mixed in water or juice. Magnesium has the added benefit of being calming and reducing stress in kids, which can be a huge component of stool holding and constipation. Start with 1/10th to 1/4 of the typical adult dose (depending on the child’s size), and increase the dose daily until it trigger a loose, borderline watery bowel movement. Most children will need to continue to use the laxative for a period of a few weeks to potentially months until they establish normal bowel habits. Always consult a physician before use. Magnesium or any other laxative should not be given if the child has true fecal impaction – it is potentially dangerous.
5. Senna tea or another “stimulating laxative.” 1) This is one of my least favorite treatments for constipation because patients often end up dependent upon the laxative to have a bowel movement. In other words – it is very difficult to stop treatment and maintain normal bowel health. Adults can drink 1 cup of “Smooth Move Tea” – older children should have 1/2 a cup of tea, and younger children should have a dose proportionate to their body weight (1/10th to 1/4 cup of tea). Always consult a physician before use. Overuse of stimulating laxatives can cause pseudomembranosis colitis.
6. Glycerine suppositories. 1) These can be helpful in infants or young children who have fecal impaction. 1) The glycerine hydrates the stool which makes it easier to pass. Remember that these can also be habit forming, especially in younger children and infants. (Many infants who require disempaction with a rectal thermometer will learn to only have a bowel movement when the thermometer is inserted – it becomes a conditioned response.)
7. Saline enema. 1) If fecal impaction is present then sometimes an enema is the only way to loosen the stool and remove the impaction. 1) It is incredibly important to use enemas correctly – they may be uncomfortable, but they should not cause pain for the child.
Directions for administering an enema: Have your child lie on his stomach with knees pulled under him, or in a hands and knees (crawling) position. Place plenty of towels underneath the child in case of leakage. Remove the protective cap and lubricate the tip of the enema with KY jelly or another lubricant. Gently slide the tip past the anal sphincter, pointing the nozzle in the direction of the child’s belly button. Push gently and follow the path of least resistance. Push the tip or nozzle 1-2 inches into the rectum. STOP if the child is in distress.
I recommend squeezing no more than a few tablespoons of solution the first time you try an enema. Squeeze the enema tube very gently to give a small, slow stream of solution into the rectum. Remove the enema tip and place the child on the toilet. If they are unable to have a bowel movement within 15 minutes then try again with another enema, using slightly more solution.
Enemas should not be used in infants unless otherwise directed by your physician.
What to do when this is not enough:
If these tricks don’t work then it is time to do a more thorough work-up with your physician.
Other causes of constipation to discuss with your doctor:
Celiac disease (relatively rare – I recommend all children to be screened for celiac disease at least once in a lifetime. Many children have few or no symptoms.)
Hypothyroidism
Lead poisoning
Rare congenital anomalies
Dysbiosis – several studies indicate gut flora imbalance leading to constipation. Bacteroides, clostridia spp and pseudomonas spp seem to be particularly involved. Naturopathic physicians can order stool microbiology testing to check for uncommon dysbiotic organisms.
Go to the doctor if:
There is severe pain along with the constipation
There is blood in the stool
After trying an enema the child still does not have a bowel movement and you suspect the stool is impacted
The child has a fever that started as the constipation started
There is a sudden change in how your child is having bowel movements (e.g., a baby usually goes every 2 hours, suddenly stops going for 2 days)
A newborn who does not pass meconium within 48 hours of birth.
References
1) Manu R Sood, FRCPCH, MD. Functional constipation in infants and children: Clinical features and differential diagnosis. UpToDate. Web. 18 March 2015.
2) Fontana M, et al. Bowel frequency in healthy children. Acta Paediatr Scand. 1989 Sep;78(5):682-4.
3) Williams CL, et al. A new recommendation for dietary fiber in childhood. Pediatrics 1995; 96:985.
4) Irastorza I, et al. Cow’s-milk-free diet as a therapeutic option in childhood chronic constipation. J Pediatr Gastroenterol Nutr. 2010 Aug;51(2):171-6. doi: 10.1097/MPG.0b013e3181cd2653.
5) Daher S, et al. Cow’s milk protein intolerance and chronic constipation in children. Pediatr Allergy Immunol. 2001 Dec;12(6):339-42.
6) Paoletti G, et al. Severe iron-deficiency anemia still an issue in toddlers. Clin Pediatr (Phila). 2014 Dec;53(14):1352-8. doi: 10.1177/0009922814540990. Epub 2014 Jul 2.
7) Indrio F, et al. Prophylactic use of a probiotic in the prevention of colic, regurgitation, and functional constipation: a randomized clinical trial. JAMA Pediatr. 2014 Mar;168(3):228-33. doi: 10.1001/jamapediatrics.2013.4367.
8) Dimidi E, et al. The effect of probiotics on functional constipation in adults: a systematic review and meta-analysis of randomized controlled trials. Am J Clin Nutr. 2014 Oct;100(4):1075-84. doi: 10.3945/ajcn.114.089151. Epub 2014 Aug 6.
9) Micklefield GH, et al. Effects of ginger on gastroduodenal motility. Int J Clin Pharmacol Ther. 1999 Jul;37(7):341-6.
10) Qin QG, et al. Acupuncture at heterotopic acupoints enhances jejunal motility in constipated and diarrheic rats. World J Gastroenterol. 2014 Dec 28;20(48):18271-83. doi: 10.3748/wjg.v20.i48.18271.
11) Zhang T, et al. Efficacy of acupuncture for chronic constipation: a systematic review. Am J Chin Med. 2013;41(4):717-42. doi: 10.1142/S0192415X13500493.
12) De Schryver AM et al. Effects of regular physical activity on defecation pattern in middle-aged patients complaining of chronic constipation.Scand J Gastroenterol. 2005 Apr;40(4):422-9.
13) Bromley D et al. Abdominal massage in the management of chronic constipation for children with disability. Community Pract. 2014 Dec;87(12):25-9.
14) Shukla R et al. Fecal Microbiota in Patients with Irritable Bowel Syndrome Compared with Healthy Controls Using Real-Time Polymerase Chain Reaction: An Evidence of Dysbiosis. Dig Dis Sci. 2015 Mar 18. [Epub ahead of print]
15) Zoppi G et al. The intestinal ecosystem in chronic functional constipation. Acta Paediatr. 1998 Aug;87(8):836-41.
Baokhinhi
September 17, 2018 at 9:58 pmGreat in-depth information!
Thanks for sharing
Stephany
October 28, 2019 at 11:34 pmThank for your share
Carol A
March 27, 2020 at 1:53 pmThanks for this page. Helpful information.
After trying the remedies listed, if he has not gone I administer a enema to him.
Give with the small rubber enema bulb syringe.
Pingback: Can I Take MiraLAX During Pregnancy – TheWetLab
November 17, 2020 at 11:19 pmPingback: Can You Be Constipated and Still Poop – TheWetLab
November 18, 2020 at 5:21 amPingback: Is It Safe to Give Kids Miralax for Constipation – TheWetLab
November 26, 2020 at 4:18 pmBrooke
August 19, 2022 at 1:29 pmAfter many searches for help with my child’s constipation, as well as going to pediatrician and gastroenterologist, this post made THE most difference. In addition to finding some good age-appropriate books, I also did a few things you mentioned here. My child now poops almost daily! Thank you so much for all the information you provided here. It’s made a world of a difference for us!